Union's 2023 State of Healthcare—a first look at the report
- Yulan Egan

- Aug 10, 2023
- 8 min read
Updated: Jul 19, 2024
At Union, we believe strongly in the power of a membership-based model—one that not only provides high-quality content, but also includes the personalized delivery of that content, access to experts, and opportunities to connect with industry peers. But we also understand that an enterprise membership might not be right for every user, at least not all of the time. To that end, we're excited to announce that we will periodically release select reports for purchase on an a la carte basis.
Up first: our 2023 State of Healthcare. We recognize how challenging it is to separate the signal from the noise in healthcare—and to move from information to insight to action. This report highlights the methodology we've developed to address this challenge head on.
It begins by first covering the meaningful (if granular) signals from the market that we think are worth paying attention to this year: data points, dates, and developments. From that curated set of signals, we distill a smaller set of core messages or insights about the state of the industry. And from those insights, we conclude with our take on a feasible number of action steps for senior executives to prioritize. Our 2023 State of Healthcare is a 50-page report covering 12 signals, 8 messages/insights, and 4 major actions for healthcare leaders.

Non-members can purchase a downloadable PDF of the report here. Existing members can access the report—and also download a ready-to-use presentation version of the content, with slide-by-slide talking points—here (please note that you must be logged in to your member account). If you'd like a sense of what you can expect, read on—we've included the first three insights from the report below.
Insight #1: MA will continue to grow in both size and strategic importance. As pressures on profitability also increase, plans will be pushed further into other parts of the value chain and providers will have to elevate their performance on value-based care.
As Medicare Advantage continues to grow in enrollment, spending, and in its strategic significance to both plans and providers, its finances are understandably attracting more attention.
In particular, the trade press and policymakers have turned a closer eye toward health plan profits from MA. When measured in terms of gross margin, MA clearly and consistently outpaces all other lines of business—by a significant margin. While this can at least be partially (or even largely) explained by the fact that per-enrollee spending is higher for MA enrollees because they’re an older, sicker, higher-utilizing population, it nonetheless has only heightened the amount of public scrutiny on MA plans. The picture is further complicated by the fact that plans have multiple potential paths to profitability in MA.
Plan payments from the federal government are determined by an annual bidding process. Plans submit premium bids which are compared to regional benchmarks that are set by CMS. As is the case with any line of business, the difference between plan premiums and costs incurred across the course of the year represent plan profits. As part of the bidding process, plans who submit bids that come in under the market benchmark receive rebates to be used to provide supplemental benefits like vision and dental coverage. Supplemental benefits which are paid for using these rebates are “mandatory” in the sense that they are provided to all plan enrollees. The plan’s premium is adjusted to account for these additional benefits, thereby providing a second potential profit lever for plans. Plans may also offer optional supplemental benefits that enrollees can choose to purchase out-of-pocket (a third profit lever). All three of these types of benefits—basic benefits, mandatory supplemental benefits, and optional supplemental benefits—are subject to Medical Loss Ratio (MLR) requirements, meaning that plan profits on these benefits cannot exceed 15%.
In recent years, an increasing number of health plans have begun to operate MA-adjacent businesses such as senior-focused care delivery services. These businesses typically serve the plan’s MA enrollees but are not subject to the MLR. As scrutiny on MA plans grow, the incentive for plans to double down on these related businesses will only increase, both as an alternate path to profits and as a means to effectively control plan costs (for example, through plan-owned value-based care providers). There is also the potential for a perverse incentive for plans to use related businesses to mask their profits and potentially exceed the MLR.
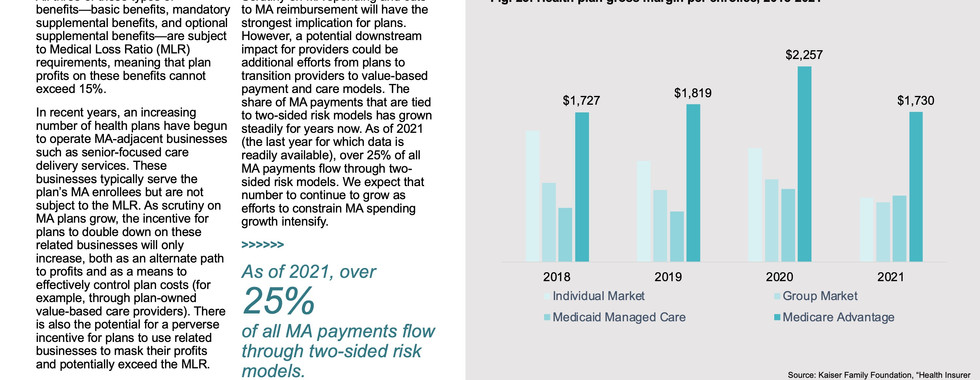
Scrutiny on MA spending and cuts to MA reimbursement will have the strongest implication for plans. However, a potential downstream impact for providers could be additional efforts from plans to transition providers to value-based payment and care models. The share of MA payments that are tied to two-sided risk models has grown steadily for years now. As of 2021 (the last year for which data is readily available), over 25% of all MA payments flow through two-sided risk models. We expect that number to continue to grow as efforts to constrain MA spending growth intensify.





Insight #2: Drug companies could push for (more) differential pricing between public and private payers, raising costs for employers in a few key segments.
Spending on drugs also continues to attract more scrutiny over time. While efforts to constrain MA spending growth have been slow and steady over time, 2022 saw the passage of a landmark drug pricing bill—one which we believe heralds a new era of drug pricing controls.
The Inflation Reduction Act (IRA) targets Medicare part D drug costs in three main ways:
Enabling price negotiation: The IRA requires the federal government to negotiate prices for some Part B/D drugs (e.g. single-source, high-spend, non-orphan) beginning in 2026.
Limiting future price increases: The IRA requires pharmaceutical companies to pay rebates if prices increase faster than inflation for drugs used by Medicare beneficiaries, beginning in 2023.
Minimizing patient exposure: The IRA caps Part D out-of-pockets costs at $2,000 a year, caps Medicare copays for insulin at $35/month, and expands eligibility for low-income subsidies and benefits.
As with any policy, the law will generate a mix of intended consequences (those detailed above) and unintended ones. For example, it could lead pharmaceutical companies to adjust patents in order to exempt certain drugs from the price negotiation program by ensuring drugs are not classified as single source. It may also lead to higher launch prices to mitigate the impact of limitations on price increases down the line.
The impacts are likely to extend beyond Medicare. We believe that the most drastic measures threatened by the pharmaceutical industry, such as the removal of drugs from the U.S. market or sweeping cuts to R&D budgets are unlikely, at least not on a large scale. It is likely, however, that pharmaceutical companies will make smaller adjustments to the R&D pipeline and process to mitigate the impacts of the law; for example, by refocusing R&D efforts on non-Medicare drugs or shifting focus away from small-molecule drugs and toward biologics.
Perhaps most critically, while proponents of the law are hopeful that the downward pressure on Medicare pricing may spill over to non-Medicare segments, we believe the law could ultimately have the opposite effect, prompting pharmaceutical companies to raise prices elsewhere—much in the same way that prices for medical services in the commercial sector are used to offset lower prices in Medicare and Medicaid. In particular, we believe that there may be efforts to raise drug prices for employers.




Insight #3: Employers will eventually struggle to absorb health cost inflation and embrace historically difficult aims—such as constraining drug spend or steerage—that limit spending growth without passing cost burdens to their employees.
For the past decade, employer medical costs have typically increased about 5% to 7% in any given year. It’s worth noting that this growth rate is relatively low by historic standards—two decades ago, the typical annual growth rate was closer to 10%.
While the precise numbers for 2022 vary by source, all agree that medical trend last year was below typical levels, by either historic or current standards, falling somewhere between 3%-5%. This is especially striking given that inflation in 2022 was at a 40-year high. But it is not especially surprising to us, for two reasons:
Employer contracts are typically renegotiated on a three-to-five-year basis, meaning that pricing updates will always lag any unexpected shifts in broader inflationary trends.
As noted earlier, the exceptionally high rate of inflation outpaced wage growth for most workers, driving historic levels of care delays which likely put a dampener on utilization.
Employers expect medical trend to return to more typical levels this year, as more commercial contracts come up for renegotiation. But the trend is not expected to match the rate of inflation seen in 2022 (at least, not yet), as downward pressures on utilization continue and, of course, because not all contracts will be up for renegotiation simultaneously.
Taking together the lower-than-usual growth in employer healthcare spend, and the fact that employers across most industries have struggled with historically high levels of turnover and job vacancies, it’s hardly surprising that employers were hesitant to cut health benefits this year. The data bears that out: most employers say that they are prioritizing benefit enhancements over efficiency efforts for 2023.
Who are these enhancements are likely to benefit the most? Given the difficulties in attracting and retaining hourly and low-wage workers, those are the groups that employers are most likely to say they are targeting for benefit enhancements.
As for how employers are enhancing benefits, many of the focus areas are intuitive. Virtual care and behavioral health are frequently-cited priorities. Women’s health has also emerged a newer focus area for enhancement efforts. In fact, most employers state not only that they are prioritizing women’s health as an important benefit enhancement lever, but that they are taking specific actions meant to address inequities in women’s health. These efforts largely focus on expanding coverage in a variety of ways. For example, an increasing number of employers are offering broad coverage for fertility benefits (i.e. not requiring employees to get a referral for fertility services). Employers are also expanding coverage for postpartum depression, women’s-focused preventive healthcare services, doula services, and group-based prenatal care. A growing number of employers are also implementing strategies meant to support under-resourced populations in particular; for example, identifying high-risk pregnancies and reducing C-section rates among historically-marginalized patient segments.
While employers may be prioritizing benefit enhancements over cost control efforts for now, that’s not to say that they are abandoning cost control efforts entirely. In fact, our study of employers suggest that they are becoming ever-more sophisticated in their efforts to improve the efficiency of their healthcare spending, in two major ways:
Employers are increasingly moving away from blunt tools such as high-deductible health plans and narrow networks which aim to constrain spending by setting large-scale, wide-ranging parameters on utilization. Instead, they’re embracing more targeted forms of cost control such as concierge navigation services, virtual-first plans, centers of excellence programs, and second opinion services. These strategies all attempt to address specific instances of high-spend (or highly-variable spend).
Employers are extending their cost control efforts from the medical space to the pharmaceutical space. Due to the incredible complexity of the pharma, pharmacy, and PBM industries, employers have been slower to adopt strategies targeting these sources of spending. But given the tremendous growth in drug spending in recent years, employers have devoted more time to understanding the inner-workings of this side of the industry. Strategies such as prior authorization requirements and limitations on drug dispensing supply are becoming increasingly common. Even more targeted strategies, such as the use of outcome-based pricing for certain drugs or the use of pharmacogenomic testing are the frontier of employer cost control efforts.
We believe the urgency for employers to adopt these strategies will only grow in the coming years, as employers’ medical costs return to and potentially even exceed recent norms.








Download a PDF of this excerpt.
Purchase the full report here.
Want more? Let's talk.
Our written report is just one way to access (and use) our state of healthcare research. Whether you're looking to educate your broader team, bring a new executive up to speed, understand your customers better, or get support for your own state of healthcare presentation, we can help. Reach out to us at info@unionhealthcareinsight.com



