Different players, different games: How healthcare’s various sectors are using AI differently in 2025
- Chris Loumeau

- Sep 12, 2025
- 9 min read
All U.S. health systems, hospitals, provider groups, life sciences organizations, and national or regional payers are racing to scale AI. But it would be a mistake to assume this surge of activity means that AI is being deployed in the same ways—or with the same level of sophistication—across the board. In reality, AI adoption and deployment varies wildly by sector, organizational size, strategic focus, and technical maturity. What health systems are trying to do with AI often looks very different from the priorities of payers, ambulatory care groups, or pharmaceutical companies. Of course, even within any given sector, resourcing and leadership choices can profoundly shape the pace and scope of progress.
This blog post explores two key dimensions of that variation: first, what each healthcare sector is primarily using AI for in late 2025—and second, where each group tends to fall along the broader maturity curve, with appropriate caveats for the heterogeneity that exists within each category. The goal isn’t to present a one-size-fits-all model, but to share some observations about patterns in how AI is being operationalized—and to shed light on what it will take to move from pilot programs to enterprise-scale impact.
By the way, the occasion for all of this was a recent update to Union’s Strategy Bootcamp on AI— our module on making sure everyone in a leadership position in healthcare can be conversant in this critical topic. Members, you can check out a recording here and materials here.
How different players are putting AI to work
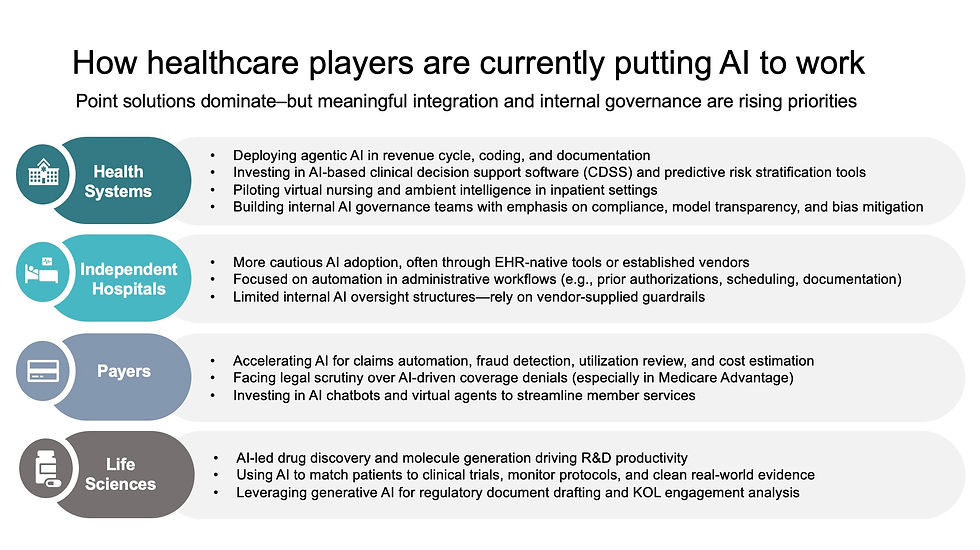
Across healthcare sectors, point solutions continue to dominate the healthcare AI adoption landscape, and players are using those point solutions for all kinds of different purposes. The result is a patchwork of AI adoption: forward momentum, yes, but fragmented use cases.
Here is a high-level summary of what we have observed in the market:
Health systems are piloting agentic tools like ambient AI scribes and virtual nursing.
Deploying AI in revenue cycle, medical coding, and clinical documentation workflows.
Investing in predictive clinical decision support and risk stratification tools.
Building internal governance teams focused on compliance, transparency, and bias mitigation.
Independent hospitals (and smaller health systems) are experimenting with AI for the same general purpose, however, rather than using points solutions, they are more often using tools embedded in their EHRs.
Focused on automating administrative workflows like prior auth, scheduling, and documentation.
Limited internal AI oversight—most rely on vendor-supplied guardrails and default settings.
Insurers are doubling down on AI-driven claims adjudication and utilization review.
Scaling AI for fraud detection, real-time cost estimation, and prior auth automation.
Facing legal scrutiny over AI-led coverage denials, especially in Medicare Advantage.
Deploying AI-powered chatbots and virtual agents for member support and navigation.
Life sciences companies are deploying generative and agentic AI to accelerate new drug discoveries and reshape regulatory workflows.
Matching patients to trials, monitoring protocol adherence, and cleaning real-world evidence.
Drafting regulatory documents and analyzing KOL engagement with gen-AI copilots.
The AI maturity journey: Pick a framework
Though each organization and sector is using AI for something a little different, in theory all are on a common journey to set up the foundational pillars needed to set up, deploy, scale, and capture ROI from any/all kinds of AI tools now and into the future.
To really get precise about this, one must pick a maturity model to use as a lens through which to look at market activity. There are quite a few available—for example, Maturity model for advancing AI governance and WillowTree’s guide to AI maturity. However, we like this organizational AI maturity framework , the “AI Maturity Roadmap”, authored by Peter Durlach, Dr. Robert Fournier, Jeremy Gottlich, Tristan Markwell, Jon McManus, Andy Merrill, and Dr. David Rhew, under the auspices of a broader AI Collaborative hosted by the Health Management Academy, Microsoft, and Nuance and first published in March 2024 in the NEJM AI. We like this one because compared to alternatives, it has been the most rigorously peer-reviewed and explicitly built for healthcare contexts.

Time for the market snapshot: Different players, different stages
If you take the NEJM AI maturity framework (or any framework) and then look at state of maturity across five major healthcare sectors: health systems, independent hospitals, ambulatory care groups, payers, and life science organizations, what you find is that overall maturity varies a lot by sector.
Here’s a summary of our view of things—again, using the NEJM framework as the lens, and adding in our own views about what’s what in each healthcare sector according to the criteria.
Let’s take the leading player first:
What we see happening in major life science organizations (i.e., Big Pharma) is that they represent the most advanced end of the AI maturity curve. From molecule generation and unique biomarker discovery to clinical trial matching and scaling regulatory documentation, AI is reshaping life-science R&D at an accelerating pace. These organizations tend to lead on strategy, talent, and infrastructure—often housing advanced data science teams and investing heavily in both generative and agentic AI. However, these enterprise efforts are not always well-integrated with clinical workflows or frontline care delivery, which can limit real-world ROI. Still, life sciences companies are the most consistently positioned in the ‘systemic’ to ‘transformational’ stages, most notably in domains like novel drug discovery, protocol development, and digital regulatory engagement.
Payers come in second in overall AI maturity in our view, having pushed maturity in strategy, operations, and data infrastructure along relatively faster than their provider counterparts. The insurer business case for AI in claims processing, fraud detection, and prior authorization automation is clear, and several national insurers have already achieved ‘operational’ or ‘systemic’ maturity in these areas. That said, clinical use cases remain more limited, and governance structures (e.g., for algorithm transparency and bias mitigation) are often reactive rather than proactive. Regulatory pressure, particularly from CMS investigations into AI-driven MA denials, has spurred greater scrutiny. As a whole, we see payers as spanning the ‘operational’ to ‘systemic’ stages across most pillars, with a few beginning to edge toward ‘transformational’ impact, specifically where AI is woven into broader member engagement strategies.
Health systems, especially large integrated delivery networks (IDNs), have emerged as some of the most visible early adopters of AI in healthcare, and also deserve credit for rolling out the most different kinds of use cases (clincial and administrative), even if still have a ways to go in organizational maturity relative to life science and payers. Many have invested in AI-powered tools for revenue cycle automation (RCM), fully integrated ambient AI scribes, and virtual nursing pilots across several clinical modalities. These initiatives reflect a growing operational fluency with agentic AI, particularly in administrative and support workflows. But despite their scale and early momentum, few health systems have successfully operationalized AI across their entire enterprise. Cultural adoption is uneven, and governance structures across multi-hospital networks remain fragmented. Most U.S. health systems today hover at the ‘operational’ stage of maturity, with only a select few achieving ‘systemic’ integration in specific areas like radiology workflows or ambient clinical documentation.
Perhaps unsurprisingly, we would put independent hospitals at an earlier phase of AI maturity because they tend to have overall less resourcing for this kind of thing and are much more cautious and conservative in their AI deployment. With smaller IT teams, more limited budgets, and fewer dedicated data science resources, these community-anchoring facilities often rely on EHR-native tools or out-of-the-box vendor solutions to streamline administrative tasks like documentation and scheduling. Adoption is more tactical than strategic. In the smallest/most resource-constrained, e.g., rural safety net hospitals, AI governance will be absent or minimal, and internal expertise is typically not yet mature enough to support more complex or custom AI deployments. On balance, many independent hospitals remain in the ‘awareness’ to ‘active’ stages of the framework: aware of AI’s promise, beginning to test limited applications, but not yet equipped to scale as ambitiously as bigger, better-resourced provider players.
Ambulatory care groups are hard to pin down because they’re so variable as a group. The category includes small practices (hey, some still exist!), as well as large multispecialty practices and physician-led ACOs, making for a dynamic and fast-changing sector. The headline here is that physician burnout and workflow inefficiencies have accelerated demand for AI scribes, digital patient intake automation, and patient engagement platforms that leverage generative AI. These solutions are often lightweight, cloud-based, and rapidly deployable—enabling faster adoption compared to inpatient settings. So uptake is relatively advanced; but, from a maturity perspective, it’s important to say that many of these AI-powered solutions operate within organizational silos, and the absence of formal governance or integrated data infrastructure limits their ability to drive cross-functional enterprise impact. This is why we would say most ambulatory care groups find themselves between the ‘active’ and ‘operational’ stages, moving quickly but very unevenly toward more mature AI integration.
Common bottlenecks: why many healthcare organizations stall on maturity
Despite the industry’s broad enthusiasm for adopting AI-powered solutions at scale, most organizations hit a maturity ceiling early in their journey. Interest is high, investment is growing, and pilot projects abound—but genuine enterprise-level scale remains elusive. Why?
First and foremost, strategy is often fragmented or poorly defined. Many organizations launch AI pilots without anchoring them to clear business or clinical goals, or without executive leadership buy-in. As a result, enthusiasm fades once the initial novelty wears off, and initiatives struggle to find long-term champions.
Second, data infrastructure continues to be a major limiting factor. While some organizations have invested in data lakes, APIs, and interoperability tools, many still operate within siloed, legacy systems that limit data liquidity. Without a robust data foundation, even the most sophisticated AI models falter in production environments.
Third, organizational AI governance remains one of the most glaring gaps. Few healthcare organizations have formal AI oversight bodies or established principles for ethical use, validation, or performance monitoring. This often results in scattered adoption and limited accountability, a dynamic that undermines trust and slows enterprise scaling efforts.
Fourth, talent and culture present persistent challenges to healthcare entities. Even when vendor solutions are available, healthcare organizations struggle to cultivate the internal expertise needed to evaluate, implement, and manage them effectively. Over-reliance on external vendors can limit learning, weaken governance, and increase long-term risk.
And finally, value realization (the ultimate barometer of AI maturity) is still more aspiration than reality for most healthcare players. Many organizations tout their AI investments, but few have clear mechanisms for tracking ROI, clinical improvement, or patient satisfaction tied to these tools. In a world where financial resources are increasingly limited and both public and regulatory scrutiny is growing, that kind of organizational ambiguity is becoming harder to justify or sustain.
What it takes to graduate to the next stage
Advancing along the AI maturity curve isn’t just about buying better tools; it’s about building a more capable, aligned, and accountable healthcare enterprise. So what does progress across a healthcare enterprise actually look like? For healthcare organizations, the first step is often creating formal structure. This includes adequately defining forward-looking roles and responsibilities for AI governance, expanding successful AI pilots into new domains, and beginning to measure outcomes (e.g., in the form of tangible workflow gains, real-world cost savings, or documentable clinical improvement). This is the phase where experimentation starts to give way to standardization.
Next phases will require deeper, more intentional investments in both technology and trust. Healthcare organizations must build or acquire fully integrated data platforms, establish cross-functional oversight councils, and ensure that enterprise AI initiatives are coordinated (not siloed) across clinical departments. Importantly, this is also when regulatory compliance and patient-facing transparency become more complex and critical.
And for those hoping to reach ‘transformational’ status, the final leap demands full organizational alignment between AI deployments and enterprise strategy. Here, AI becomes not just a tool, but a core organizational capability—natively embedded in everything from clinical pathways and revenue optimization to R&D and patient engagement strategies. Healthcare organizations at this stage are not merely users of AI; they are shapers of its future.
Some promising examples are beginning to emerge. Mayo Clinic has developed internal teams dedicated to clinical validation of AI tools. Tempus is redefining how genomic data and AI can intersect at scale. And national payers are starting to treat AI as a critical infrastructure layer for optimizing risk, cost, and consumer experience. These leaders offer early blueprints, but the road ahead remains long for most.
Conclusion: maturity is a meaningful AI differentiator
In a healthcare landscape increasingly saturated with AI tools, the real differentiator isn’t technology adoption, it’s organizational maturity. Everyone is buying. Everyone is piloting. But not everyone is prepared to scale. It's important to keep our eye on the ball of organizational AI maturity, not just individual solutions or overall uptake. Organizations need to build real capabilities in order for AI to transform healthcare workflows, deliver its promised value, and finally solve some of the industry’s biggest paint points.
Remember: Our newest Strategy Bootcamp is now available
Union members, don’t forget to check out the update to our Healthcare AI Strategy Bootcamp module recording and materials. We actually didn’t even get into AI maturity in that—the new module focuses on getting everyone up to speed with the newest AI terms, policy developments, players to know, and more. You can access it all from the Union website’s ‘education’ section. And don’t forget to register for the next strategy bootcamp, which will be on revenue cycle.


